
TL;DR:
- Hospital-grade cleaning is a regulated standard requiring effective disinfectants, proper application, and thorough documentation. It emphasizes validated contact times, pathogen kill levels, and rigorous procedures like terminal cleaning to ensure infection control in regulated environments. Implementing digital governance, proper staff training, and careful product evaluation are essential for achieving and maintaining compliance.
Hospital-grade cleaning is not simply about using stronger products than you would at home. It is a rigorously defined standard that dictates which disinfectants are used, how they are applied, and whether the entire process is documented for compliance. For facilities managers in healthcare, aged care, childcare, and other regulated environments, understanding what is hospital-grade cleaning means understanding a system of infection control, not just a product category. This article unpacks the regulatory foundations, operational realities, and practical implementation steps that separate genuine hospital-grade practice from cleaning that merely looks thorough.
Table of Contents
- Key takeaways
- What hospital-grade cleaning actually means
- Operational realities that determine cleaning effectiveness
- Cleaning protocols for hospitals and regulated facilities
- Technology and data-driven cleaning governance
- Choosing the right products and providers
- My perspective on getting hospital-grade cleaning right
- How Just About Cleaning supports your compliance goals
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Hospital-grade means registered efficacy | Disinfectants must be proven effective against specific baseline pathogens, not just marketed as strong. |
| Contact time is non-negotiable | Wiping a surface dry before the dwell time expires renders even the best disinfectant ineffective. |
| Documentation is part of compliance | Cleaning logs, training records, and Safety Data Sheets are audited alongside physical cleaning results. |
| Technology is reshaping governance | Digital dashboards and occupancy sensors are replacing manual logs as the new compliance standard. |
| Training and culture drive outcomes | Product selection matters far less than whether staff apply products correctly and consistently. |
What hospital-grade cleaning actually means
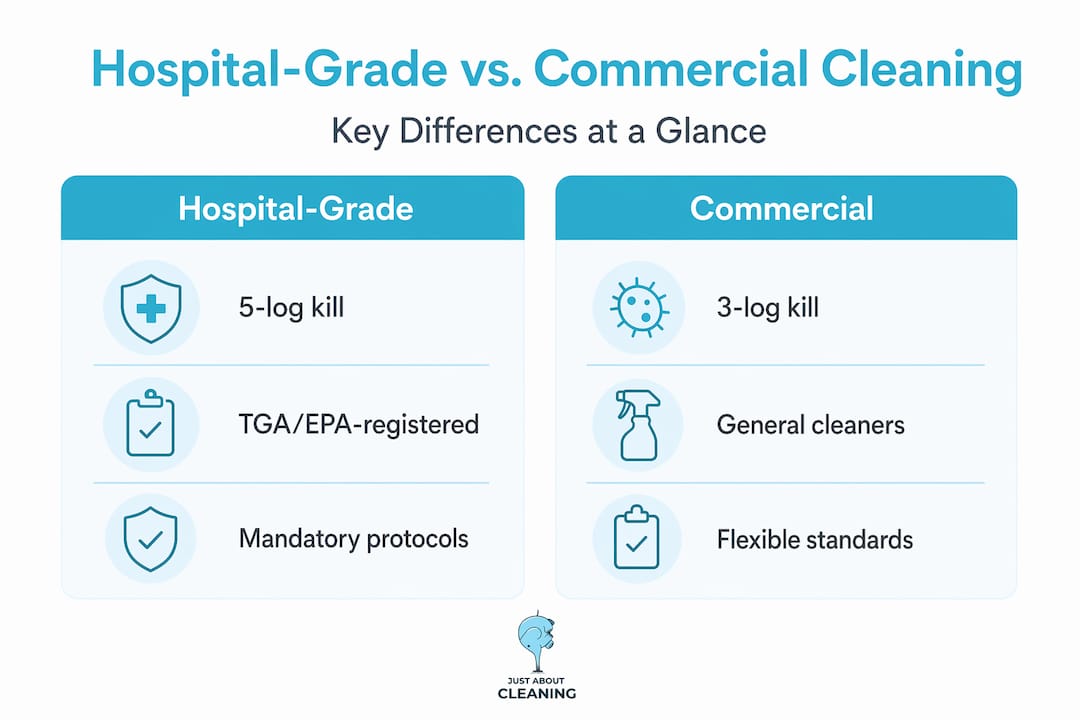
The term "hospital-grade" carries regulatory weight, not just marketing appeal. At its core, a hospital-grade disinfectant must be registered as effective against a defined set of baseline pathogens: Staphylococcus aureus, Salmonella enterica, and Pseudomonas aeruginosa. These three bacteria represent a cross-section of Gram-positive and Gram-negative organisms, making them a reasonable benchmark for broad-spectrum performance.
Beyond pathogen kill claims, hospital-grade disinfectants are formulated to achieve what the industry refers to as 5-log kill standards, eliminating 99.999% of target organisms. That figure differentiates hospital-grade products from general commercial cleaners, which typically achieve 3-log or 4-log reductions.
It is worth clarifying three terms that are often used interchangeably but carry distinct meanings in a clinical or regulated facility context.
- Cleaning removes visible soil, organic matter, and surface debris. It is a prerequisite for effective disinfection but does not kill pathogens.
- Sanitising reduces microbial load to a level considered safe by public health standards. It is appropriate for food service but not sufficient for healthcare.
- Disinfecting destroys or inactivates a defined range of pathogens on surfaces. Hospital-grade disinfection targets a broader and harder-to-kill range than standard commercial products.
In Australia, product selection and use must also align with relevant standards, including the Therapeutic Goods Administration (TGA) requirements for disinfectants used in clinical settings and guidance from the Australian Commission on Safety and Quality in Health Care. Internationally, the US EPA registration framework provides a widely referenced benchmark for what constitutes a hospital-grade product.
| Classification | Pathogen kill level | Typical application |
|---|---|---|
| General commercial cleaner | 3-log (99.9%) | Offices, retail, general public spaces |
| Sanitiser | 3-log to 4-log | Food preparation surfaces |
| Hospital-grade disinfectant | 5-log (99.999%) | Healthcare, aged care, clinical facilities |
| Sterilant | 100% destruction of all organisms | Surgical instruments, sterile fields |
Operational realities that determine cleaning effectiveness
Here is where many facilities programmes fall short. The biggest compliance gap in hospital sanitation practices is not product quality. It is contact time, also called dwell time.

Disinfectant contact time refers to the period a surface must remain visibly wet with disinfectant for the active ingredient to kill the target pathogen. Contact times typically range from 3 to 10 minutes depending on the product and organism. The problem is that most cleaning staff wipe surfaces dry within 30 to 60 seconds, which means the disinfectant never has the opportunity to work.
It compounds further when you consider that contact time varies by pathogen. A product's shortest listed contact time may apply only to easier-to-kill organisms. For harder pathogens like Norovirus or Clostridioides difficile spores, the required dwell time may be considerably longer. If your facility has a risk profile that includes these pathogens, the label's headline contact time is not the number you should be working from.
Pro Tip: When evaluating disinfectants, ask the supplier for the contact time specific to the highest-risk pathogens in your environment. If that figure is not available or not validated, the product may not meet your actual compliance needs.
Several other operational factors reduce real-world disinfectant efficacy, even when the correct product is in use:
- Organic load: Residual blood, bodily fluids, or food debris on a surface will neutralise disinfectant before it reaches the pathogen. The two-step process, clean first then disinfect, exists for this reason.
- Surface type and porosity: Porous or rough surfaces hold more bioburden and are harder to disinfect uniformly.
- Product dilution errors: Ready-to-use concentrates are often mixed incorrectly, either too weak to be effective or so concentrated that they are corrosive and leave residue.
- Staff workflow pace: High-volume cleaning environments create pressure to move quickly, which compresses dwell times below the validated threshold.
The misconception that stronger chemicals alone guarantee results is widespread in both healthcare and facilities management. Effective hospital-grade cleaning depends on correct application methodology, not product concentration alone.
Cleaning protocols for hospitals and regulated facilities
Implementing genuine infection control cleaning requires more than good products. It requires defined procedures, clear frequency schedules, and thorough documentation.
The standard two-step process for hospital-grade cleaning works as follows:
- Remove physical soil. Use a detergent solution and clean cloth to wipe away visible debris, dust, and bioburden. This step is non-negotiable because residual organic matter deactivates disinfectant.
- Apply disinfectant and maintain contact time. Apply the approved disinfectant product to the surface and allow it to remain wet for the full validated dwell time. Do not wipe dry prematurely.
- Follow a zone-based or risk-based order. Clean from the least contaminated area to the most contaminated. In a patient room, this means starting with surfaces furthest from the patient and finishing with high-touch zones like bed rails, call buttons, and tap handles.
- Document the cleaning activity. Record the time, product used, surfaces covered, and the staff member responsible. This log is a compliance artefact, not optional paperwork.
- Conduct terminal cleaning after patient discharge. Terminal cleaning is a high-intensity disinfection protocol distinct from routine daily cleaning. It covers all surfaces in a room, including walls and ceiling vents, and requires its own documented procedure with Safety Data Sheets and training records.
Pro Tip: For facilities outside of hospitals that are applying hospital-grade standards, such as aged care or childcare, use the terminal cleaning protocol template as your baseline for deep clean events. It gives you a defensible, audit-ready record even when a regulatory body is not actively monitoring your environment.
PPE use and staff training are mandatory under any credible hospital-grade cleaning programme. Gloves, eye protection, and appropriate gowning are required when handling concentrated disinfectants or cleaning in high-risk zones. Training must be documented and revisited regularly, not just conducted during onboarding.
It is also worth noting that facilities commonly fail audits due to documentation failures rather than physical cleaning shortfalls alone. Inspectors assess cleaning logs, training records, chemical safety documentation, and competency assessments alongside the physical condition of a space. For a practical starting point on building a compliant cleaning programme, a healthcare compliance checklist can help you identify documentation gaps before they become audit findings.
Technology and data-driven cleaning governance
The future of hospital-grade cleaning compliance is digital. Manual cleaning logs, while still required by many frameworks, are increasingly supplemented or replaced by real-time monitoring systems.
Digital cleaning governance using occupancy sensors, live dashboards, and electronic task management tools allows facilities managers to align cleaning activity with actual site usage rather than fixed schedule assumptions. A room that has been used three times between scheduled cleans poses a different risk profile than one that has remained unoccupied.
The benefits for facilities managers are practical and measurable:
- Compliance evidence is generated automatically and is audit-ready in real time.
- Resource allocation improves because cleaning effort is directed to where it is needed, not where it was planned weeks earlier.
- Trends in compliance performance become visible across multiple sites, allowing proactive intervention.
- Contract accountability improves because performance data can be shared with commissioners or accreditation bodies.
Accreditation bodies and commissioners now demand digital visibility into cleaning performance as a condition of contract and accreditation in a growing number of frameworks. Facilities relying solely on paper-based records are already behind the standard that healthcare estates are moving toward. Understanding how cleaning audits drive compliance outcomes is a key part of building this governance capability.
Choosing the right products and providers
Selecting a hospital-grade disinfectant, or a cleaning provider that uses them, requires looking beyond the label. The label tells you what the product can do under optimal laboratory conditions. Your job is to assess whether it performs under real-world conditions in your facility.
When evaluating products, ask for evidence on three specific criteria: contact time for your highest-risk pathogens, kill spectrum coverage (bacteria, viruses, and fungi relevant to your site), and real-world validation data, not just laboratory studies. A supplier who cannot provide these should not be supplying your healthcare or regulated environment.
When assessing cleaning contracts and service providers, the same rigour applies:
- Confirm that cleaning staff have documented competency in applying hospital-grade disinfectants correctly, including dwell time compliance.
- Require the provider to supply cleaning logs, incident records, and training verification as part of the service agreement.
- Ask specifically how they handle terminal cleaning and what their procedure looks like, including the documentation trail.
- Verify that PPE protocols are in place and enforced, not just described in a policy document.
Pro Tip: Request a mock audit of your cleaning programme before a formal inspection. A provider who resists or cannot produce audit-ready documentation on short notice is showing you exactly what an inspector will find.
For facilities managers looking to benchmark their cleaning programme against current Australian compliance expectations, a clear picture of top cleaning standards in 2026 is a useful reference point.
My perspective on getting hospital-grade cleaning right
Having worked closely with facilities teams across healthcare, aged care, and commercial environments, I have seen the same failure pattern repeat: a facility invests in premium disinfectants, briefs staff, and then assumes the work is done. It rarely is.
What I have come to understand is that contact time non-compliance is primarily a workflow problem, not a training problem. Staff are under time pressure, rooms need to turn over, and waiting ten minutes for a disinfectant to dwell is genuinely difficult in a high-throughput environment. The more practical fix is selecting a product with a shorter validated contact time for your specific pathogen risk profile. That is a procurement decision that removes the workflow barrier entirely.
I have also seen facilities invest in rigorous physical cleaning and then fail audits because their paperwork was in disarray. Proper documentation is as critical as the physical act of cleaning. An inspector cannot verify what was not recorded.
My honest view on data-driven governance: it is not a nice-to-have. If your facility has more than one site or more than 20 staff involved in cleaning, manual logs cannot give you the visibility you need to manage compliance proactively. Invest in a digital system early. The cost is far lower than a failed audit or a healthcare-associated infection event.
— David
How Just About Cleaning supports your compliance goals
If this article has clarified what hospital-grade cleaning requires, the next practical question is whether your current cleaning programme actually meets those requirements. Just About Cleaning partners with healthcare facilities, aged care providers, medical centres, and regulated commercial environments across Australia to deliver cleaning services built around compliance, documentation, and trained staff.
Just About Cleaning's medical facility cleaning services are structured around the same principles covered in this article: correct disinfectant selection, verified dwell time procedures, terminal cleaning protocols, and audit-ready documentation. The team is trained onsite, operates to documented standards, and is equipped to support your compliance posture rather than create a burden for it. If your facility needs a cleaning partner that understands infection control cleaning as a system, not just a service, reach out to Just About Cleaning to discuss your requirements.
FAQ
What does hospital-grade cleaning mean?
Hospital-grade cleaning refers to a cleaning standard that uses EPA-registered or TGA-approved disinfectants effective against specific baseline pathogens, applied according to validated contact time and documented procedures. It is defined by the process and compliance framework, not just the product used.
How is hospital-grade cleaning different from regular commercial cleaning?
Hospital-grade cleaning requires disinfectants that achieve a 5-log (99.999%) kill rate against a broader pathogen spectrum, plus formal documentation, PPE use, and terminal cleaning protocols. Regular commercial cleaning typically targets a 3-log reduction and does not carry the same compliance or documentation obligations.
Why does contact time matter so much in hospital-grade cleaning?
Contact time is the period a disinfectant must remain on a surface to kill target pathogens. Wiping a surface dry too early renders the disinfectant ineffective regardless of its chemical strength, making contact time adherence one of the most critical and commonly missed steps in hospital sanitation practices.
What surfaces and areas require terminal cleaning?
Terminal cleaning is performed after patient discharge and covers all surfaces in a room, including walls, vents, and high-touch points. It is a distinct, high-intensity protocol separate from routine daily cleaning and must be fully documented with logs, training records, and Safety Data Sheets.
How can facilities managers verify their cleaning meets hospital-grade standards?
Facilities managers should review disinfectant product labels for pathogen-specific contact times, audit documentation practices against compliance requirements, and assess staff competency records. Engaging a provider who offers audit-ready cleaning logs and transparent protocols is the most reliable way to confirm compliance.